Medicare Appeal Form For Providers
CMS-855A for Institutional Providers. Ad Form CMS-855B More Fillable Forms Register and Subscribe Now.
Po Box 14020 Lexington Ky 40512 Fill Out And Sign Printable Pdf Template Signnow
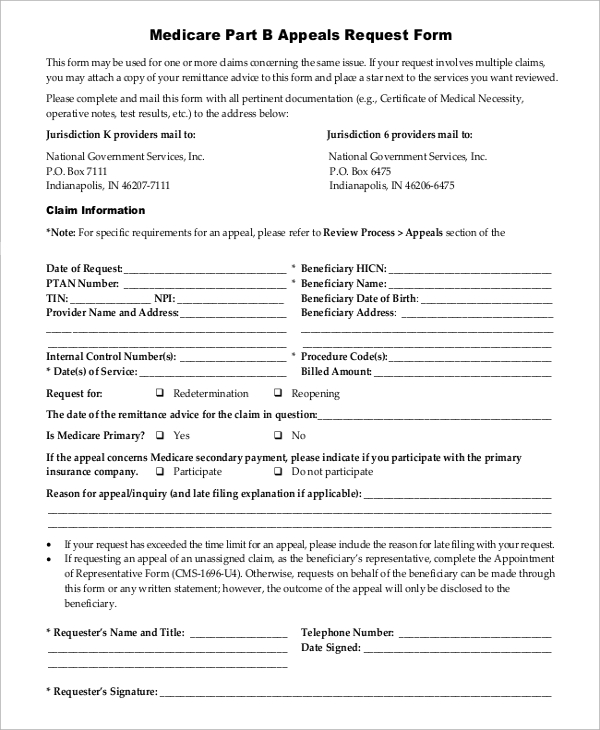
Appeals must be submitted using the following forms.
Medicare appeal form for providers. Authorization to Disclose Personal Health Information. Your right to a fast appeal. Compare plans or attend our online or in-person seminars for more details.
Medicare member payment appeal post service PDF If you have a dispute around a payment you would have received under original Medicare please send your dispute documentation of what original. Beneficiarys name First Middle Last Medicare number. Many issues or concerns can be promptly resolved by our Member Services Department.
Or download the form from Medicares website. CENTERS FOR MEDICARE MEDICAID SERVICES. Service Dates Initial Denial Notification Dates.
Request for redetermination of Medicare prescription drug denial pdf Use this form to request. Accelerated Payments to Providers. I want to request a hearing by an Administrative Law Judge ALJ because Im not satisfied with the decision made during the 2nd level of my appeal Request for Administrative Law Judge ALJ Hearing or Review of Dismissal formOMHA-100.
If you are dissatisfied with any aspect of your healthcare plan Customer Care your provider or treatment facility you can submit a grievance at any time. Fill out a Redetermination Request Form PDF 100 KB and send it to the company that handles claims for Medicare. Ad See how our 2022 Medicare plans offer a total approach to wellness with extra benefits.
A copy of the original claim. Grievances do not include. It describes how providers physicians and suppliers apply the appeals.
Learn how to get a fast appeal for Medicare-covered services you get that are about to stop. Fill out the Medicare Reconsideration Request form CMS-20033. CMS-855I for Physicians and Non-Physician Practitioners.
Understand your Medicare options rights and protections. If you have questions about appointing a representative. CMS-855R for Reassignment of Medicare.
Appointment of Representative Form CMS-1696. The PAR Form is used for all provider inquiries and appeals related to reimbursement. Claim ID Number s Reference NumberAuthorization Number.
Providers participating physicians and other suppliers have the right to appeal claim decisions. If you missed the deadline for appealing you may still file an appeal and get a decision if you can show good cause for missing the deadline. Administrative Simplification Compliance Act Waiver Request Form.
If you received a Medicare Redetermination Notice MRN on this claim DO NOT use this form to request further appeal. Keep a copy of everything you send to Medicare as part of your appeal. Ad See how our 2022 Medicare plans offer a total approach to wellness with extra benefits.
Date the service or item was received mmddyyyy Item or service you wish to appeal. Compare plans or attend our online or in-person seminars for more details. If you have not already done so you may want to first contact Member Services before submitting an appeal.
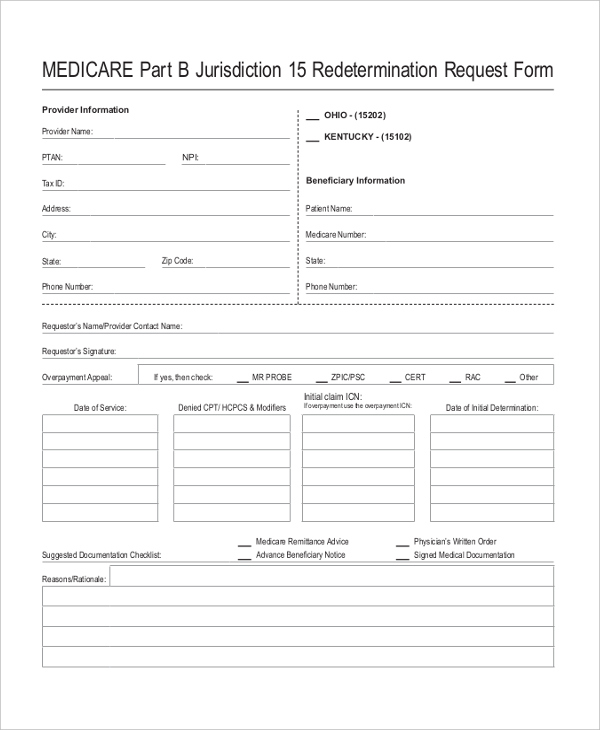
If an enrollee would like to appoint a person to file a grievance request a coverage determination or request an appeal on his or her behalf the enrollee. Appeals and Grievances. MEDICARE RE DETERMINATION REQUEST FORM 1st LEVEL OF APPEAL.
Advance Beneficiary Notice of Noncoverage CMS-R-131 Advance Payments to Providers. This request should include. If you received a message MA-130 on the Medicare Remittance Notice for this claim no appeal.
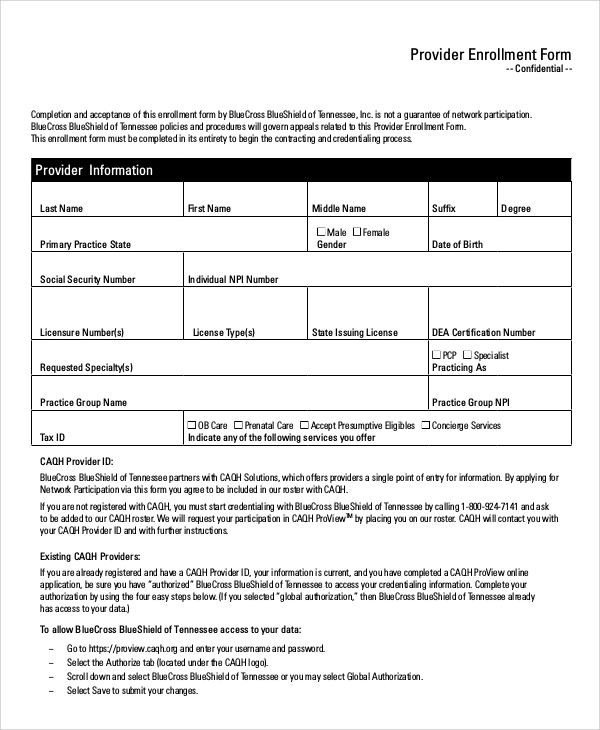
The representative a form or written request with your appeal request to the Medicare Administrative Contractor MAC the company that handles claims for Medicare or your Medicare health plan. Provider Forms Guides. The following forms can be used for initial enrollment revalidations changes in status and voluntary termination.
In order to request an appeal of a denied claim you need to submit your request in writing within 60 calendar days from the date of the denial. This booklet doesnt cover Medicare Parts C or D appeals. Provider Action Request Form.
1-800-MEDICARE Authorization to Disclose Personal Health Information. Your next level of appeal is a Reconsideration by a Qualified Independent Contractor QIC - Form. Visit the Forms Needed for Your Level 3 Appeal at HHSgov and fill out the OMHA-100 the Request for Hearing by an Administrative Law Judge ALJ Hearing or Review of Dismissal form.
Appointment of Representative Form. This link takes you away from the Fallon Medicare Plus website Part D appeal form Use this online form to start a Medicare Part D appeal. You may use this form to appeal multiple dates of service for the same member.
Access a form so that someone who helps you with your Medicare. Appeals for nonparticipating providers. We are currently in the process of enhancing this forms library.
Provider Appeal Correspondence Address. CMS-855B for Clinics Group Practices and Certain Other Suppliers. Customer Date of Birth.
Applying for an Extended Repayment Schedule. Easily find and download forms guides and other related documentation that you need to do business with Anthem all in one convenient location. This booklet tells health care providers about Medicares 5 appeal levels in Fee-for-Service FFS original Medicare Parts A B and includes resources on related topics.
During this time you can still find all forms. REQUEST FOR APPEAL OR CLAIM DISPUTESRECONSIDERATIONS. Providers may request corrective adjustments to any previous payment using this form.
You must file your appeal by the date in the MSN.
Amerigroup Appeal Form Fill Out And Sign Printable Pdf Template Signnow
Coventry Advantra Provider Appeal Form Fill Online Printable Fillable Blank Pdffiller
Free 10 Sample Medicare Forms In Pdf Ms Word
Free 10 Sample Medicare Forms In Pdf Ms Word

Namm California Dispute Form
Free 8 Sample Medicare Forms In Ms Word Pdf
2
Aarp Appeal Form Fill Online Printable Fillable Blank Pdffiller

Epmg Medicare Appeal Grievance Form
Free 8 Sample Medicare Forms In Ms Word Pdf

Amerigroup Appeal Form Fill Online Printable Fillable Blank Pdffiller
2
Aetna Medicare Plans Complaint And Appeal Form

Epmg Appeal Grievance Form

Example Part B Redetermination Request Form Medicare Payment Reimbursement Cpt Code Icd Denial Guidelines
Wellcare Appeal Form Fill Out And Sign Printable Pdf Template Signnow
Medicare Reconsideration Form Fill Online Printable Fillable Blank Pdffiller
Redetermination Reopening Form Tutorial Je Part B Noridian

Medicare Provider Forms